Bcbs Formulary Exception Form
Bcbs Formulary Exception Form - (please specify all medication[s]/strengths tried, length of trial and reason for. The following documentation is required. ________________________ / ______ / ___________________________________ Web you may request an exception to your prescription medication coverage for drugs that are not included on your prescription drug list. Verify the member’s eligibility and benefits. To submit request electronically, please go to mail:
Make sure the member has active coverage with this plan and has benefit coverage for the service you are requesting. Web you and your doctor can submit an exception request for drug coverage. ________________________ / ______ / ___________________________________ first mi. To submit request electronically, please go to mail: Medicare supplement insurance plan documents.
Web to submit a formulary or tiering exception, use the forms below: Medicare supplement insurance plan documents. Please consult your plan brochure for formulary coverage. To submit request electronically, please go to covermymeds.com using plan/pbm name “bcbs nc”. Please note the following restrictions;
270 Bcbs Forms And Templates free to download in PDF

Web complete the following steps prior to submitting a medical policy coverage exception request: Submit an online fe or pa request via the covermymed’s free web portal (for prime therapeutics to review). Web you and your doctor can submit an exception request for drug coverage. Web if you are uncertain whether a drug requires prior authorization or a formulary exception.
Fillable Online Value Formulary Exception Prior Authorization Request

Web to submit a formulary or tiering exception, use the forms below: View these forms and documents in spanish. Web if you are requesting a copay exception for more than one medication, please use a separate form for each medication. Web complete the following steps prior to submitting a medical policy coverage exception request: Incomplete forms will be returned for.
Fillable Online FORMULARY EXCEPTION REQUEST FORM University of Utah
To submit request electronically, please go to mail: View these forms and documents in spanish. Please note the following restrictions; Only the prescriber may complete this form. Web if you are requesting a copay exception for more than one medication, please use a separate form for each medication.
Fillable Online Prior Authorization / Formulary Exception Request Form

Web for formulary exception (fe) and prior authorization (pa) requests for drugs covered under a member’s pharmacy benefit, providers can: To submit request electronically, please go to covermymeds.com using plan/pbm name “bcbs nc”. Web find medicare advantage plan, medicare advantage dual care plan (hmo snp), prescription drug plan and medicare supplement insurance plan forms and documents you need to help.
Form Frx004 Formulary Exception Request Form printable pdf download

Web to submit a formulary or tiering exception, use the forms below: ________________________ / ______ / ___________________________________ 1) indicate all the drug name(s) the patient has failed on in this class: To request coverage of a medication that's not on the plan formulary (list of covered drugs), you can ask for a formulary exception. ____ / ____ / ______.
Bcbs Formulary Exception Form - Web complete the following steps prior to submitting a medical policy coverage exception request: (please specify all medication[s]/strengths tried, length of trial and reason for. Therapeutic failure(s) with generic and/or brand medications in this therapeutic class. Only the prescriber may complete this form. Web if you are uncertain whether a drug requires prior authorization or a formulary exception request, see the precertification lists and pharmacy utilization management criteria in our medical policy. Submit an online fe or pa request via the covermymed’s free web portal (for prime therapeutics to review). To submit request electronically, please go to covermymeds.com using plan/pbm name “bcbs nc”. Web you and your doctor can submit an exception request for drug coverage. Web find medicare advantage plan, medicare advantage dual care plan (hmo snp), prescription drug plan and medicare supplement insurance plan forms and documents you need to help you manage your medicare plan. Web indicate the outcome that best describes your patient’s experience with all drugs in this therapeutic class:
Verify the member’s eligibility and benefits. To submit request electronically, please go to covermymeds.com using plan/pbm name “bcbs nc”. Medicare supplement insurance plan documents. To submit request electronically, please go to covermymeds.com using plan/pbm name “bcbs nc”. Web prescription drug formulary exception.
To submit request electronically, please go to mail: Web indicate the outcome that best describes your patient’s experience with all drugs in this therapeutic class: Web find medicare advantage plan, medicare advantage dual care plan (hmo snp), prescription drug plan and medicare supplement insurance plan forms and documents you need to help you manage your medicare plan. Web if you are requesting a copay exception for more than one medication, please use a separate form for each medication.
1) indicate all the drug name(s) the patient has failed on in this class: Web if you are requesting a copay exception for more than one medication, please use a separate form for each medication. Web find medicare advantage plan, medicare advantage dual care plan (hmo snp), prescription drug plan and medicare supplement insurance plan forms and documents you need to help you manage your medicare plan.
To request coverage of a medication that's not on the plan formulary (list of covered drugs), you can ask for a formulary exception. Web prescription drug formulary exception. ____ / ____ / ______.
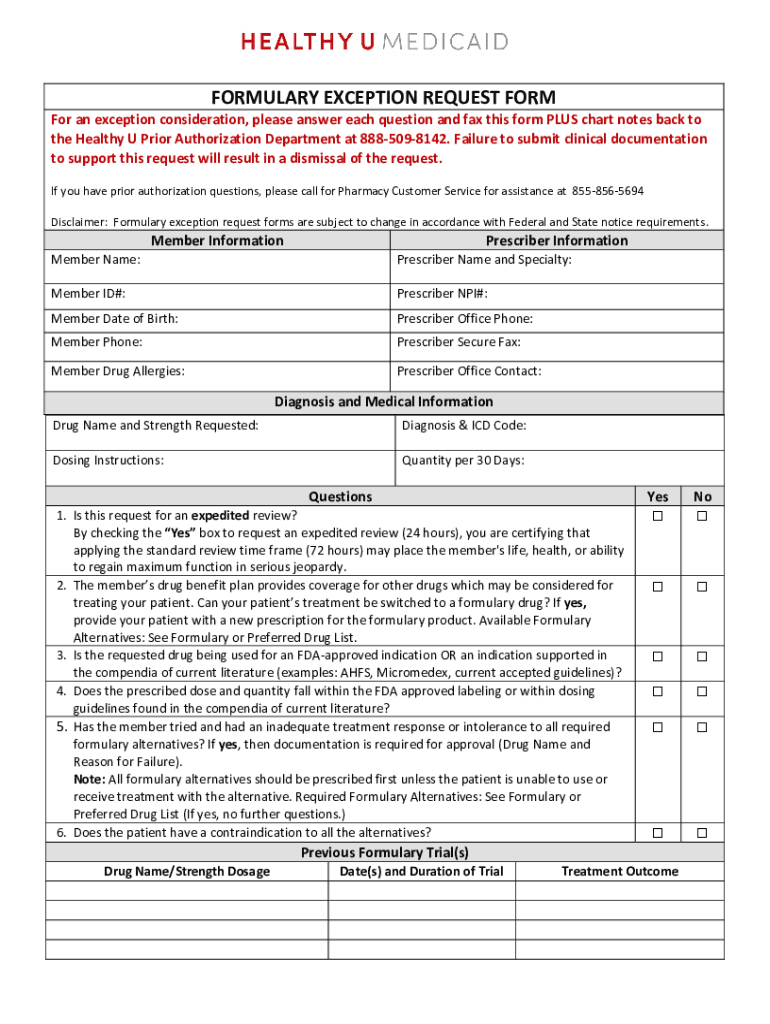
To Request Coverage Of A Medication That's Not On The Plan Formulary (List Of Covered Drugs), You Can Ask For A Formulary Exception.
Web if you are requesting a copay exception for more than one medication, please use a separate form for each medication. Web if a member chooses to change plans during the benefit year exception approvals may no longer be valid. Incomplete forms will be returned for additional information. Medicare supplement insurance plan documents.
Web If You Are Requesting A Copay Exception For More Than One Medication, Please Use A Separate Form For Each Medication.
To submit request electronically, please go to mail: ________________________ / ______ / ___________________________________ first mi. Make sure the member has active coverage with this plan and has benefit coverage for the service you are requesting. Web to request coverage of a medication that's not on the plan formulary (list of covered drugs), you can ask for a formulary exception.
Web You May Request An Exception To Your Prescription Medication Coverage For Drugs That Are Not Included On Your Prescription Drug List.
Web find medicare advantage plan, medicare advantage dual care plan (hmo snp), prescription drug plan and medicare supplement insurance plan forms and documents you need to help you manage your medicare plan. Web for formulary exception (fe) and prior authorization (pa) requests for drugs covered under a member’s pharmacy benefit, providers can: Only the prescriber may complete this form. ________________________ / ______ / ___________________________________
Web Here Are Some Of The Common Documents And Forms You May Need In Order To Treat Our Members And Do Business With Us.
Please note the following restrictions; To submit request electronically, please go to covermymeds.com using plan/pbm name “bcbs nc”. ____ / ____ / ______ patient name: View these forms and documents in spanish.